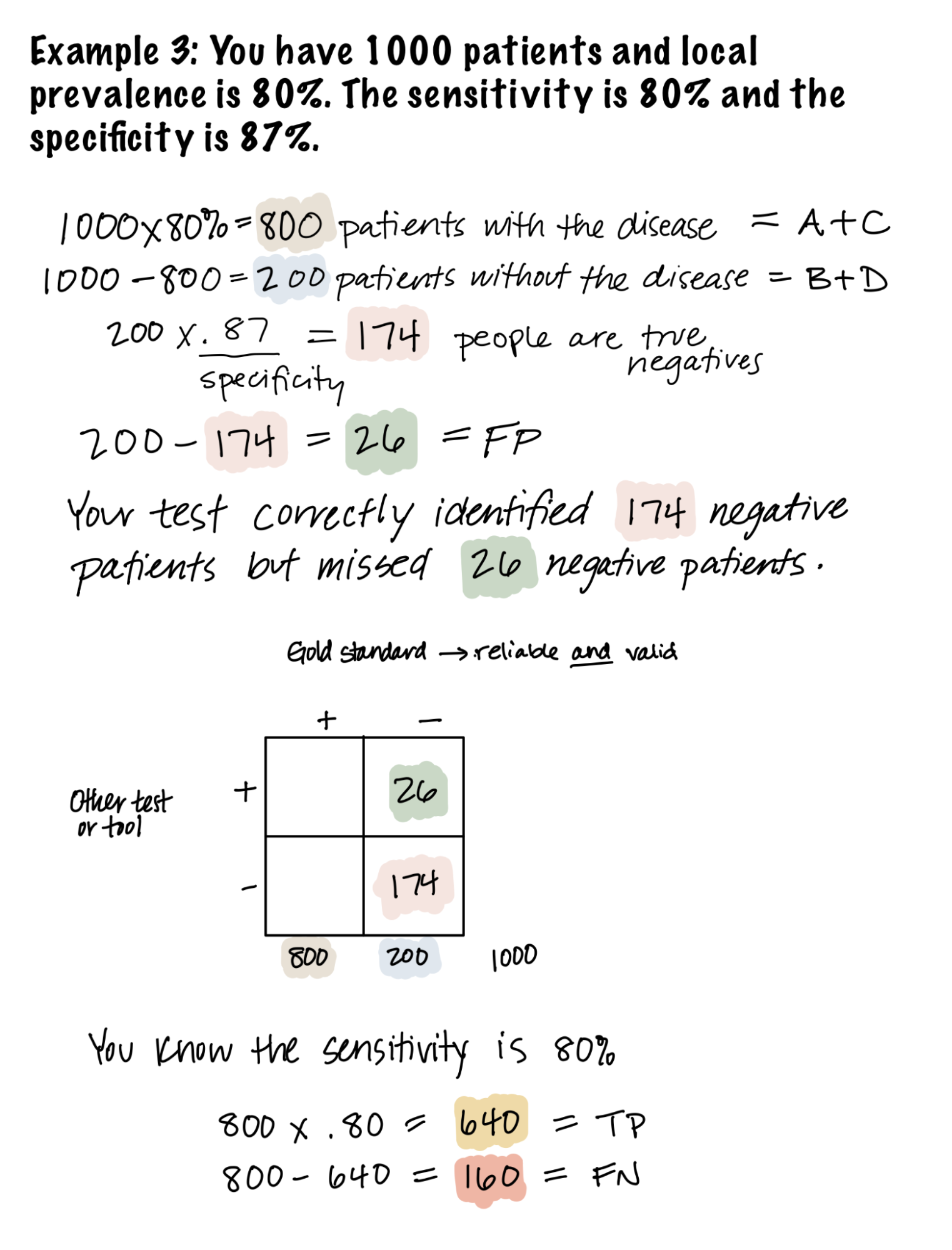
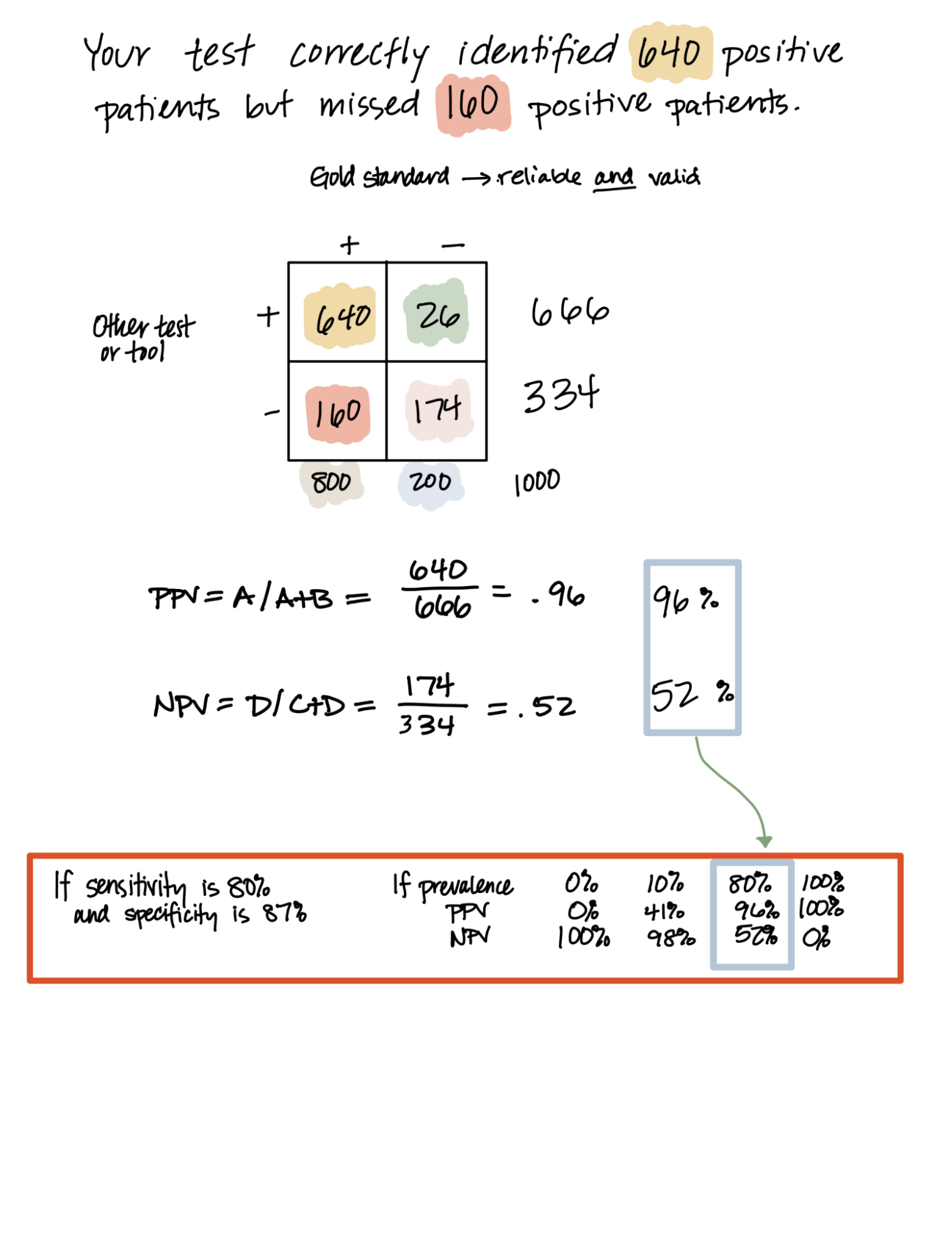
Study Guide: Diagnostics and Screening

Epidemiology Copyright © 2023 by Charlotte Baker is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.